Robotic Assisted Laparoscopic Prostatectomy
About
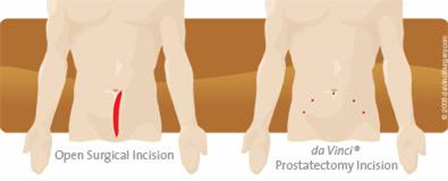
Prostatectomy is the surgical removal of the prostate gland as a treatment for prostate cancer. To do this we now use a surgical robot called the Da Vinci to facilitate this. This enables us to do complex laparoscopic or “key hole” surgery as opposed to the traditional open surgery.
The robot is controlled by the surgeon at all times and doesn’t work independently. The robot is connected to the patient and very small instruments are inserted through key holes in the abdominal wall. The surgeon sits at a separate console and does the operation without touching the patient. The surgeon has complete control of the robot at all times.
Kent and Canterbury is the first hospital in South East England, outside of London, to offer this advanced treatment option.
Is the surgeon able to do the same operation with the robot?
Yes.
In terms of cancer treatment it is regarded as the same as open surgery and doesn’t compromise cancer control.
What are the advantages of robotic surgery?
This type of surgery offers many advantages for the surgeon and for the patient.
- Highly magnified high definition view of operation
- Complete 3D view
- Much finer more delicate dissection
- Far more precise surgery
- Abolishes tremor
- Lower complication rate
- Lower infection rate
- Less pain
- Quicker recovery
- Shorter hospital stay
- Shorter catheter time
- Less blood loss and a lower rate of needing a blood transfusion (1%)
- Earlier return to work/normal daily activities
- Improved cosmetic result
Are there any complications of this surgery?
- Bruising in the scrotum or around the wounds
- Bladder spasms/pain with catheter
- Constipation – this is important to avoid and you will be given medication for this
- Blood in the urine
- Urinary or wound infection
- Facial swelling lasting a few hours
- Shoulder pain lasting a few hours
- Bleeding requiring transfusion or need to return to theatres (1%)
- Damage to structures around the prostate i.e. bowel/rectum/bladder/blood vessels or ureters (tubes between kidney and bladder) (<1%)
- Risk of clots in the legs(DVT) or clots on the lungs(PE) (1%). You will have injections to reduce this problem. Keeping well hydrated and early mobilisation/walking helps prevent this problem.
- Medical complications such as chest infections or MI(<1%)
- Conversion to an open operation – again this is rare at around 1%
- Incontinence
- Continence can be affected by this treatment however longterm(longer than a year) incontinence that requires further surgical treatment is around 2%. Majority of patients will have some degree of incontinence when the catheter is removed and may need to use pads for a period of time. With robotic surgery continence recovers quicker. It is important to do your pelvic floor exercises before during and after your recovery.
- Erectile dysfunction
- Erections can be affected by this surgery, this is more likely in older patients and if you have weak erections before the surgery. In patients who want to keep their erections we can offer “nerve spare” surgery. This is part of the operation where we protect the nerves that go down to the penis, these run very close to the prostate and can be gently peeled off. We don’t offer this in patients with more advanced disease. Even with nerve spare surgery erections are not guaranteed. You will be given a daily tablet to help the erections recover, in some men this can take between 1 year and 18 months.
Are there any alternatives to this treatment?
Yes. These should have been discussed with you by your Urologist or Oncologist. Depending on your age, PSA, type of disease and other health issues, radiotherapy, brachytherapy, surveillance or hormone therapy are all treatment options. However this type of surgery is only chosen if we feel it’s the most appropriate treatment option for you.
Can the robot breakdown?
Potentially although this is a very rare scenario(<0.5%). If this happens either the operation can be rescheduled or the operation is done as an open operation. Over 4000 robots are being used worldwide and this has only been reported in a handful of cases.
How long does the operation take?
Around 2 hours. It is done under general anaesthetic, and you will wake up in the recovery bay before being transferred back to the ward. Operation times can vary depending on various factors such as obesity, size of Prostate and previous abdominal surgery.
What happens from now?
Once we have decided on robotic surgery you will be contacted with a date for the operation. You will be asked to attend the pre-assessment clinic where routine bloods and ECG are taken and an assessment of your fitness for surgery is made.
You will then be admitted to the hospital on the morning of the operation, where you will meet the surgeon, the anaesthetist and the nursing staff. You will be asked to sign the consent form. You will have one enema administered before the operation.
After surgery
No. the operation shouldn’t affect your libido.
It will however affect your fertility, you will have no ejaculate following the operation and in some men they notice a small degree of penile shortening.
When can I start sexual relations?
There is no restriction on resuming sexual relations after the catheter is removed once you and your partner are happy to do so.
No. Robotic surgery is less painful than open surgery. Before you wake up the anaesthetist give you pain relief and we use local anaesthetic (numbing) in the wounds and bladder. If you feel you have pain then please inform the nursing staff so they can give you analgesia.
A lot of patients wake up with the sensation of a full bladder or can get periodical bladder spasms. This is because of the catheter and the surgery around the bladder, and not because the bladder is full. It usually settles but if not can be helped with medication.
1 day. The majority of patients are discharged the day after the operation. Along with the catheter you wake up with a drain tube which is removed prior to discharge.
Yes. Before leaving hospital you will be given instructions on how to manage with the catheter and manage dressings.
Absorbable stitches are used so no stitches need to be removed.
You will be given pain killers to take as and when you need them, medication to prevent constipation and a daily tablet for the erections to start once the catheter is removed.
If needed district nurse, community continence team or additional follow up appointments can be arranged. The ward can be called if there are any problems.
Initially exercise should be gentle but gradually built up on a daily basis as symptoms allow. Don’t confine yourself to bed. You should take a full and balanced high fibre diet and maintain a good fluid intake especially in the first week.
Occasional alcohol consumption is ok but should be restricted in the first week after the operation.
Energy levels can vary from day to day following this surgery.
The catheter is a very important part of your recovery. It protects the join between your bladder and your urethra(water pipe) in the early stages of the healing process. We like to leave the catheter for a short as time as possible, between 7 – 10 days after the operation. Removal of the catheter is very straight forward and only takes a matter of seconds however it is done in the Urology department. You should have been given a date for catheter removal before you leave the hospital.
Once the catheter is removed please continue doing your pelvic floor exercises regularly.
Remember most patients have some degree of leakage initially once the catheter is removed and you may need to use pads for a period of time. The community continence team can help with pads.
This varies between patients. You will only be fit to drive if you can do an emergency stop without it causing pain. A minimum of one week.
Again this is variable. You can return to work when you feel able. Some patients are back after one week, others take 3-4 weeks. It is important only to do light duties initially and no heavy lifting for 4 weeks.
Short haul 2 weeks. Long haul 4 weeks. These are just minimum recommendations and again if you have any concerns please delay you travel. You must also check with your carrier and travel insurance company.
Results
This takes our pathologists about 2 weeks to process and examine the prostate. The results can be phoned to you once we receive them.
Most patients don’t need any other forms of treatment. Some patients with more advanced disease may be offered radiotherapy after the surgery, either immediately or later if there is a rise in the PSA, others may be given a long course of hormones. This will be discussed with you.
After the initial pathology results, you will be seen by the surgeon at six weeks after the surgery, then at 3 monthly intervals with a check PSA. If all is well then the appointments can be stretched to six months. You may also have appointments with the physio’s if there is an issue with recovery of continence or in the Erectile Dysfunction clinic if restoration of the erections is important to you.
How do we improve our service?
We are constantly trying to improve the high quality care we provide. We continually audit and assess our results. We will ask you to fill out questionnaires on incontinence, erectile dysfunction and overall quality of life. We would like you to fill these out before the operation and at all your follow up appointments. We also want to you to record the first day you manage without pads and when you return to work. Please let us know these dates at follow up or by email.
All this information is handled anonymously, and is collected on all patients. Please feel free to add any other comments whether good or bad. All these comments will be taken seriously and will be used to improve the system further.